Abstract
Crohn’s disease (CD) is an idiopathic chronic inflammatory bowel disease that can affect any part of the gastrointestinal tract (GIT), though it most commonly involves the terminal ileum and colon. Duodenal involvement is rare, accounting for only 0.5%–4% of cases, and isolated duodenal CD is even less common, occurring in fewer than 0.07% of patients. This report describes a 37-year-old female with a long history of CD presenting with progressive duodenal stenosis and associated symptoms such as epigastric pain, weight loss, and vomiting. Despite medical therapy with biologics, including adalimumab and ustekinumab, the disease progressed, leading to the need for surgical intervention. The patient underwent an innovative surgical procedure involving antrectomy, resection of the first, second, and third portions of the duodenum, Roux-en-Y gastrojejunostomy, cholecystectomy, and total pancreas preservation. Histopathological analysis confirmed the diagnosis of CD with chronic transmural inflammation, non-caseating granulomas, and lymphoid follicle formation. Postoperatively, the patient experienced significant clinical improvement, with good nutritional recovery and no recurrence of symptoms during follow-up. This case highlights the challenges in managing rare and severe manifestations of CD, particularly when medical therapy is insufficient. Surgical intervention is often reserved for complications such as obstruction, perforation, or intractable symptoms. The described surgical approach deviated from traditional methods like Whipple’s procedure, focusing instead on preserving the pancreas and minimizing GIT disruption. This innovative technique proved effective, underscoring the importance of tailoring surgical strategies to individual patient needs.Given the rarity of duodenal CD and the paucity of literature on its management, this report adds valuable insights into the potential for conservative surgical approaches to improve outcomes while reducing morbidity. Further studies are warranted to explore optimal strategies for treating this uncommon presentation of CD.
1. Introduction
Crohn's disease (CD) is an inflammatory bowel disease that can affect the entire gastrointestinal tract (GIT)
, which is an entity that comprises a heterogeneous spectrum of intestinal and extraintestinal manifestations
, so it can involve any part of the gastrointestinal tract from the mouth to the anus
| [3] | Song DJ, Whang IS, Choi HW, Jeong CY, Jung SH. Crohn’s disease confined to the duodenum: A case report. World J Clin Cases [Internet]. 2016; 4(6): 146. Disponível em: http://dx.doi.org/10.12998/wjcc.v4.i6.146 |
[3]
, characterized by irregular granulomatous inflammation of the entire thickness of the intestine
.
The incidence of CD is 5 to 10 per 100,000 people per year and the prevalence is 50 to 100 per 100,000 people
, in addition most patients with gastroduodenal CD have concomitant lesions in the terminal ileum or colon, but the disease Isolated Crohn's gastroduodenal is an extremely rare presentation of the disease, accounting for less than 0.07% of all CD patients
| [3] | Song DJ, Whang IS, Choi HW, Jeong CY, Jung SH. Crohn’s disease confined to the duodenum: A case report. World J Clin Cases [Internet]. 2016; 4(6): 146. Disponível em: http://dx.doi.org/10.12998/wjcc.v4.i6.146 |
[3]
, so although CD can involve any part of the alimentary tract, duodenal involvement is a clinical entity rare that occurs in only 0.5-4.0% of patients
| [4] | Racz JM, Davies W. Severe stricturing Crohn’s disease of the duodenum: A case report and review of surgical options. Int J Surg Case Rep [Internet]. 2012; 3(7): 242–5. Disponível em: http://dx.doi.org/10.1016/j.ijscr.2012.03.012 |
[4]
, being reported for the first time by Gottlieb and Alpert in 1937
.
Symptoms of gastroduodenal CD include epigastric pain, dyspepsia, early satiety, anorexia, nausea, vomiting and weight loss
| [3] | Song DJ, Whang IS, Choi HW, Jeong CY, Jung SH. Crohn’s disease confined to the duodenum: A case report. World J Clin Cases [Internet]. 2016; 4(6): 146. Disponível em: http://dx.doi.org/10.12998/wjcc.v4.i6.146 |
[3]
, clinical presentation that depends on the part of the GI tract affected. The most frequent symptoms of duodenal CD are abdominal pain, weight loss, nausea and vomiting, and tend to reflect progressive gastric outlet obstruction. Early satiety occurs in more than 60%. Upper gastrointestinal bleeding that manifests as hematemesis or melena occurs in less than 20%
.
Surgery is required in approximately 70% of patients with Crohn's disease
, and unfortunately, 30-70% of all patients require repeated operations
. However, medical management has evolved greatly during the last decade: innovations have included the introduction of new therapeutic agents for the prophylaxis and management of complications
.
This case report describes a 37-year-old female patient with stenosing CD in the upper gastrointestinal tract, involving the second portion of the duodenum. In this case, the surgical procedure was: antrectomy + resection of the 1st, 2nd and 3rd portion of the duodenum + Roux-en-Y gastroenteroanastomosis + cholecystectomy + pancreas preservation. In addition, a literature review was carried out and no reports of similar procedures were found in the English and Portuguese literature (MEDLINE, LILACS, SCIELO, COCHRANE).
2. Case Presentation
A 37-year-old female patient, followed up in the health system since 2013 (32 years old) for diarrhea, oral ulcers, abdominal pain, vomiting and weight loss. She reports that symptoms started at age 18, without bothering her much, until age 30 (2011). She denies diabetes or high blood pressure. She denies using alcohol or smoking.
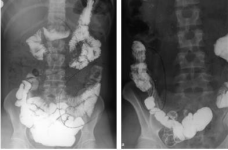
Figure 1. Transit and morphology of the small intestine.
In 2014, an examination of transit and morphology of the small intestine was performed, which showed changes suggestive of CD in the duodenum and jejunum- ileal transition [
figure 1]. After this diagnosis, she started treatment with Adalimumab, with a dose of 40mg every 14 days, with improvement and control of symptoms.
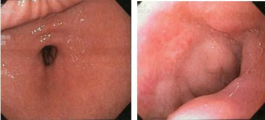
In 2015, there was a recurrence of the underlying disease, with the presentation of canker sores in the oral cavity, anal fissures, diarrhea and weight loss. From that time, we have the record of an upper digestive endoscopy (UDE), which showed marked gastric stasis, with great inflammatory and ulcerated involvement of the duodenum with severe stenosis [
figure 2].
Figure 2. Upper digestive endoscopy.
In 2016, the disease was well controlled, with few symptoms and fecal calprotectin < 30.
In 2017, clinical symptoms returned, and at that time the use of immunobiological treatment with Adalimumab was intensified for weekly intervals with the same dosage. After 3 months of treatment, there was no clinical improvement, when a new UDE was performed, which showed persistence of signs of inflammation. Fecal calprotectin exceeded the value of 1800 and so, it was chosen to change the medication from Adalimumab to Ustekinumab, which was used until 2018.
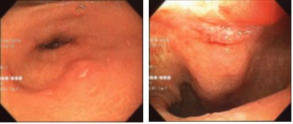
In April 2018, with the diagnosis of moderate/severe Crohn's Disease, with Crohn's Disease Activity Index > 300, and more severe weight loss, at that moment, a contrast radiography of the esophagus, stomach and duodenum (ESD) and an UDE were performed. showed, respectively, stenosis of the second portion of the duodenum and bulb ulcer with duodenal stenosis [
figure 3]; as well as a colonoscopy that showed sessile polyps in the rectum, sigmoid and colon, in addition to signs of sigmoid colitis.
Figure 3. Upper digestive endoscopy.
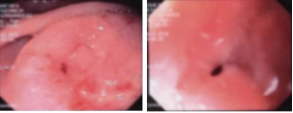
In August 2018, two UDEs were performed, which showed an active ulcer in the middle bulbar portion [
figure 4] and scarring stenosis in the 2nd duodenal portion and gastric food stasis. Due to duodenal stenosis and progressive weight loss, a food jejunostomy was performed in October of the same year.
Figure 4. Upper digestive endoscopy.
In December 2018, a new UDE, shows the poorly distensible, deformed bulb, at the expense of scar retraction in the transition to the second portion, and a fusiform ulcer with flat edges, covered by fibrin, is still observed. In the post-pyloric portion of the bulb, on the right anterolateral wall, an active ulcer is also observed, covered by a thick layer of fibrin. The transition to the second portion is carried out with difficulty. Duodenal ulcers: a1 of sakita and h1 of sakita; duodenal substenosis.
In 2019, an UDE was performed to tattoo the duodenal stenosis area with India ink, to aid in the indicated surgical procedure, Whipple's surgery, scheduled for February of that year.
In January 2019, the surgical procedure was performed, initially with the perspective of performing the Whipple technique, but the following was performed: Antrectomy + resection of the 1st, 2nd and 3rd portion of the duodenum + Roux-en-Y gastroenteroanastomosis + Cholecystectomy + exploration of bile ducts, open technique as described below: Supra and infra umbilical median laparotomy approximately 25 cm long. A large size retractor was placed as show on [
figure 5].
Figure 5. Supra and infraumbilical median laparotomy.
Then, a broad Kocher and Cattell maneuver was performed to explore the duodenum, which was tattooed at the site of the stenosis. After that, a duodenotomy was performed in the 3rd portion, to palpate the lesion, followed by a cholecystectomy and catheterization of the main bile duct with a 6Fr catheter. Until the exit of the same in the papilla of Vater.
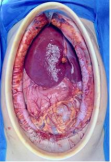
Thus, it was confirmed that the lesion was above the papilla and it was decided to perform a duodenal resection with preservation of the pancreatic head. The duodenum was dissected along with the head of the pancreas with ligation of the peri- pancreatic vessels. At that time, the 3rd portion of the duodenum was sectioned using a Stapler 45mm power with two blue loads and cranially folded. The catheterized papilla was observed through the duodenum and this was achieved with a stapler + 3 blue loads. Reinforcement suture was performed with 4.0 polypropylene on continuous suture [
figure 6].
Figure 6. Laparotomy showing pancreas and excluded duodenum.
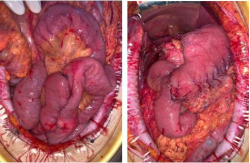
In the following time, a Schoemaker antrectomy was performed, preserving the Latarjet nerve (for this, a stapler with +5 golden loads was used). Next, the anterior jejunostomy loop was released and a one layer suture was performed, inverting the anterior suture line with 4.0 polypropylene in continuous suture. About 40 cm from the Treitz, the handle was sectioned with the same stapler + 01 blue load. The loop mesentery was elongated to construct the Roux-Y. A gastro-jejunal, retro-colic, end- to-side anastomosis was performed with polidioxanona 3.0 thread in continuous suture. At 60 cm from the anastomosis, a side to side enteroenteric anastomosis was performed with 4.0 polypropylene in continuous suture [
figure 7].
Figure 7. Roux-en-Y on the left and gastrojejunal anastomosis on the right.
The procedure time was 7 hours and the patient was discharged on day 7th. After that, she was discharged in good clinical condition.
At the end of 2019, 19 blades and 19 blocks with histopathological material were sent for review and confirmation of Crohn's disease at a referral center in São Paulo, Brazil.
The histopathological procedure, performed in January 2020, found in a segment of the duodenum: chronic transmural ulcerated duodenitis; formation of lymphoid follicles, outline of a fistulous path, foci of abscess and cryptitis; Acute chronic serositis with outline of non-caseating epithelioid granulomas with multinucleated giant cells. Absence of parasites. In addition to small bowel segment: chronic transmural enteritis with focal cryptitis; acute chronic serositis with formation of non-caseating epithelioid granulomas with multinucleated giant cells; presence of blackened pigment of exogenous origin compatible with endoscopic tattooing. Absence of parasites. Thus, the examination concludes that the findings may correspond to inflammatory bowel disease of the Crohn's type, in correlation with clinical history and absence of history of previous surgical procedure.
Initial follow-up was carried out monthly, progressing to quarterly and after every six month. So far, the patient is doing well clinically, with good acceptance of the oral diet, well from a nutritional point of view and with regaining part of the lost weight. In addition, she continues to use immunobiological treatment with Ustekinumab.
3. Discussion and Conclusions
CD is a chronic intestinal disorder of multifactorial etiology that can cause varied symptoms and complications
| [4] | Racz JM, Davies W. Severe stricturing Crohn’s disease of the duodenum: A case report and review of surgical options. Int J Surg Case Rep [Internet]. 2012; 3(7): 242–5. Disponível em: http://dx.doi.org/10.1016/j.ijscr.2012.03.012 |
[4]
, being observed mainly in the age group of 30 to 40 years and with a male to female ratio of 1.2:1.0
.
The disease rarely affects the stomach and duodenum, and the gastroduodenal frequency varies between 0.5% and 4.0% in all CD patients
| [3] | Song DJ, Whang IS, Choi HW, Jeong CY, Jung SH. Crohn’s disease confined to the duodenum: A case report. World J Clin Cases [Internet]. 2016; 4(6): 146. Disponível em: http://dx.doi.org/10.12998/wjcc.v4.i6.146 |
[3]
. Thus, although it can occur in any part of the alimentary tract, involvement of the duodenum is rare and severe narrowing of the duodenum is even less common
| [4] | Racz JM, Davies W. Severe stricturing Crohn’s disease of the duodenum: A case report and review of surgical options. Int J Surg Case Rep [Internet]. 2012; 3(7): 242–5. Disponível em: http://dx.doi.org/10.1016/j.ijscr.2012.03.012 |
[4]
.
Patients with duodenal involvement usually have CD that affects other areas of the GIT and, therefore, most cases occur in association with each other
| [4] | Racz JM, Davies W. Severe stricturing Crohn’s disease of the duodenum: A case report and review of surgical options. Int J Surg Case Rep [Internet]. 2012; 3(7): 242–5. Disponível em: http://dx.doi.org/10.1016/j.ijscr.2012.03.012 |
[4]
, but CD confined to the duodenum or stomach without involvement of the small intestine or colon is very rare and occurs in less than 0.07% of all CD patients
| [3] | Song DJ, Whang IS, Choi HW, Jeong CY, Jung SH. Crohn’s disease confined to the duodenum: A case report. World J Clin Cases [Internet]. 2016; 4(6): 146. Disponível em: http://dx.doi.org/10.12998/wjcc.v4.i6.146 |
[3]
. Due to this rarity, the first report of duodenal involvement of this pathology was described by Gottlieb and Alpert in 1937, and Ross reported the gastric alteration for the first time in 1949
| [3] | Song DJ, Whang IS, Choi HW, Jeong CY, Jung SH. Crohn’s disease confined to the duodenum: A case report. World J Clin Cases [Internet]. 2016; 4(6): 146. Disponível em: http://dx.doi.org/10.12998/wjcc.v4.i6.146 |
| [4] | Racz JM, Davies W. Severe stricturing Crohn’s disease of the duodenum: A case report and review of surgical options. Int J Surg Case Rep [Internet]. 2012; 3(7): 242–5. Disponível em: http://dx.doi.org/10.1016/j.ijscr.2012.03.012 |
[3, 4]
.
Diagnosis of gastroduodenal disease requires a high level of clinical suspicion
| [3] | Song DJ, Whang IS, Choi HW, Jeong CY, Jung SH. Crohn’s disease confined to the duodenum: A case report. World J Clin Cases [Internet]. 2016; 4(6): 146. Disponível em: http://dx.doi.org/10.12998/wjcc.v4.i6.146 |
[3]
as its diagnosis should be considered as a differential from all duodenal lesions, especially if the patient has other manifestations of inflammatory bowel disease (IBD) in the GI tract
. In most cases, the clinical picture suggests peptic ulceration, which may be associated with weight loss, diarrhea, and perhaps fever
.
Radiographic diagnosis of CD can be suspected when long tubular segments of duodenal narrowing with superficial mucosal ulcerations are seen
, in addition the endoscopic findings of this IBD are irregular erythematous granular mucosa, multifocal erythematous patches, friability and varying degrees of ulceration. of the stomach and irregular thick duodenal folds, cobblestone appearance, polypoid and polypoid lesions and focal ulceration of the duodenum
| [3] | Song DJ, Whang IS, Choi HW, Jeong CY, Jung SH. Crohn’s disease confined to the duodenum: A case report. World J Clin Cases [Internet]. 2016; 4(6): 146. Disponível em: http://dx.doi.org/10.12998/wjcc.v4.i6.146 |
[3]
.
In UDE, the identification of granulomas in the biopsy is the most important step in confirming the disease
| [3] | Song DJ, Whang IS, Choi HW, Jeong CY, Jung SH. Crohn’s disease confined to the duodenum: A case report. World J Clin Cases [Internet]. 2016; 4(6): 146. Disponível em: http://dx.doi.org/10.12998/wjcc.v4.i6.146 |
[3]
, as duodenal dysfunction may resemble other lesions, such as tuberculosis, syphilis, histoplasmosis, lymphoma, primary carcinoma, metastatic disease, sarcoid, trauma or pseudolymphoma
. However, endoscopic biopsies usually do not reveal granulomas because the tissues of these biopsies are usually confined to the mucosa
| [3] | Song DJ, Whang IS, Choi HW, Jeong CY, Jung SH. Crohn’s disease confined to the duodenum: A case report. World J Clin Cases [Internet]. 2016; 4(6): 146. Disponível em: http://dx.doi.org/10.12998/wjcc.v4.i6.146 |
[3]
.
Thus, if there are no defined histological findings, gastroduodenal CD can still be diagnosed by a comprehensive clinical evaluation, including detailed history taking, physical examination, radiological findings, endoscopic evaluation, and histological and laboratory investigations
| [3] | Song DJ, Whang IS, Choi HW, Jeong CY, Jung SH. Crohn’s disease confined to the duodenum: A case report. World J Clin Cases [Internet]. 2016; 4(6): 146. Disponível em: http://dx.doi.org/10.12998/wjcc.v4.i6.146 |
[3]
.
In addition, radiological examination using double contrast media is useful in cases with strictures, especially in advanced diseases, in addition to a barium enema that should be performed in suspected cases of gastrocolic fistula
| [7] | Ingle SB, Adgaonkar BD, Jamadar NP, Siddiqui S, Hinge CR. Crohn’s disease with gastroduodenal involvement: Diagnostic approach. World J Clin Cases [Internet]. 2015; 3(6): 479–83. Disponível em: http://dx.doi.org/10.12998/wjcc.v3.i6.479 |
[7]
.
Thus, the treatment of the pathology is mainly medical therapy, with surgery generally reserved for complications
, with the first line of treatment in active gastroduodenal CD being a proton pump inhibitor in combination with steroids
| [8] | Wagtmans MJ, Verspaget HW, Lamers CB, van Hogezand RA. Clinical aspects of Crohn’s disease of the upper gastrointestinal tract: a comparison with distal Crohn’s disease. Am J Gastroenterol. 1997; 92(9): 1467–71. |
[8]
. Some studies have demonstrated steroid-induced remission in active disease.
Likewise, 6-Mercaptopurine and Azathioprine proved to be useful in maintaining steroid-induced remission
| [7] | Ingle SB, Adgaonkar BD, Jamadar NP, Siddiqui S, Hinge CR. Crohn’s disease with gastroduodenal involvement: Diagnostic approach. World J Clin Cases [Internet]. 2015; 3(6): 479–83. Disponível em: http://dx.doi.org/10.12998/wjcc.v3.i6.479 |
[7]
.
Otherwise, surgical treatment is indicated in patients who are clinically unresponsive
| [7] | Ingle SB, Adgaonkar BD, Jamadar NP, Siddiqui S, Hinge CR. Crohn’s disease with gastroduodenal involvement: Diagnostic approach. World J Clin Cases [Internet]. 2015; 3(6): 479–83. Disponível em: http://dx.doi.org/10.12998/wjcc.v3.i6.479 |
[7]
or who have massive and persistent upper gastrointestinal bleeding, gastric outlet obstruction, and fistula or abscess formation
| [7] | Ingle SB, Adgaonkar BD, Jamadar NP, Siddiqui S, Hinge CR. Crohn’s disease with gastroduodenal involvement: Diagnostic approach. World J Clin Cases [Internet]. 2015; 3(6): 479–83. Disponível em: http://dx.doi.org/10.12998/wjcc.v3.i6.479 |
[7]
, or in addition to intractable pain
, duodenal obstruction being the most important indication for surgical resolution
. In the largest published series, obstruction was the indication for surgery in 77% of patients and intractable pain in 18%
.
Thus, once the need for surgical intervention is established, the surgical strategy will vary depending on the intestinal portion affected by this IBD
, as the procedures can be resection or bowel sparing procedures
, however, it is essential, in First, surgery preserves intestinal absorption capacity, as well as avoids obstructive and perforating disease, without disturbances and obtaining the shortest margins in case of intestinal resections. For this reason, stricturoplasty techniques should be preferred over resection techniques to ensure both bowel preservation and protection against recurrence
.
Thus, options for the surgical treatment of complicated duodenal alteration include bypass, resection, or stricturoplasty. Extended strituroplasty with pedunculated jejunal patch repair has also been described
. However, modern surgical treatment of small bowel CD is based on well-established principles of bowel conservation through bowel-sparing procedures and minimization of gross resection margin
.
Traditionally, the gold standard operation for the treatment of obstructive duodenal disease has been bypassed without resection, via gastrojejunostomy. Ross et al. published the longest follow-up of patients treated with bypass for obstruction of duodenal CD. After a 14-year follow-up, 70% of the patients required reoperation for complications directly related to the disease. Complications included marginal ulceration, recurrent obstruction, and duodenal fistulas. Malignant degeneration was not observed in this series and is extremely rare but has been reported previously
. In addition to the gold standard, several surgical procedures have been advocated for the treatment of gastroduodenal pathology. For example, gastrojejunostomy with or without vagotomy was the most used procedure in the past.
Based on the location of the disease, gastroduodenostomy or duodenojejunostomy were also used as bypass procedures
.
By-pass procedures are associated with acceptable perioperative morbidity but carry a significant risk of long-term complications, including delayed gastric emptying in up to 24% of patients and marginal ulceration after gastrojejunostomy, occasionally requiring the need for additional surgery
.
In view of this, stricturoplasty
, popularized by Lee and Papiaoannu in the 1970s and refined further by Alexander Williams
| [4] | Racz JM, Davies W. Severe stricturing Crohn’s disease of the duodenum: A case report and review of surgical options. Int J Surg Case Rep [Internet]. 2012; 3(7): 242–5. Disponível em: http://dx.doi.org/10.1016/j.ijscr.2012.03.012 |
[4]
, has been advocated as an alternative to circumvent procedures in selected patients. Heineke-Mikulicz pyloroplasty can be used in patients with short stenosis of the first, second and third portions of the duodenum; Finney's strit stricturoplasty is better suited to longer strictures in the first and fourth parts of the duodenum
.
Given the variability of duodenal Crohn's disease, only a limited number of studies on its surgical procedures have been published and few data describe the existing optimal treatment
| [4] | Racz JM, Davies W. Severe stricturing Crohn’s disease of the duodenum: A case report and review of surgical options. Int J Surg Case Rep [Internet]. 2012; 3(7): 242–5. Disponível em: http://dx.doi.org/10.1016/j.ijscr.2012.03.012 |
[4]
.
Therefore, in our case report, the failure of clinical treatment with immunobiological drugs, in addition to progressive duodenal stenosis, evidenced in UDE over the years, we chose to perform pancreatoduodenectomy, the Whipple technique, seeking to remove the part affected by CD. Intraoperatively, we chose to perform an atypical technique, in which we sought to preserve the jejunum and the head of the pancreas, performing a duodenotomy to locate the lesion, confirmed to be above the papilla of Vater, then duodenal resection and pancreatic preservation were performed total. Finally, we concluded with the making of a Roux Y and the gastrojejunal anastomosis. Thus, we seek to minimize damage to the GIT and improve the patient's quality of life.
The procedure performed, in the clinical and operative context reported, is an innovative method, in which the total preservation of the pancreas was the chosen option. The technique proved to be valid and safe, with a good postoperative and follow-up result for the patient.